ScribeWiz
The procedure report, built as the procedure happens.
ScribeWiz is MedNext's procedure-reporting engine for gastroenterology.
As the doctor reviews and acts on each finding during a gastroscopy or colonoscopy, ScribeWiz turns those clinical decisions into a complete, doctor-specific procedure report covering diagnosis, findings, and ICD coding.
The report is ready the moment the patient leaves theatre, with no typing after the fact and no dictation backlog.

Core Features
What ScribeWiz delivers.
Built Around the Procedure
The moment a gastroscopy or colonoscopy is booked, ScribeWiz knows which procedure it is and only presents the relevant clinical branches, such as upper findings for a gastroscopy and lower findings for a colonoscopy.
Click-Built Clinical Findings
Doctors select findings from branching, specialty-specific menus, including polyps, gastritis, mucosal changes, and more, with each selection pulling in pre-approved clinical text and structured detail like lesion size.
Doctor-Specific Report Templates
Every gastroenterologist's report reads the way they write it. Templates and wording are configured per doctor, from concise summaries to longer-form letters, and can be updated on request.
Automatic ICD Coding
Each clinical finding carries its own ICD code behind the scenes, so the statutory reporting hospitals must submit to state health departments is generated automatically, with no manual coding by nursing staff.
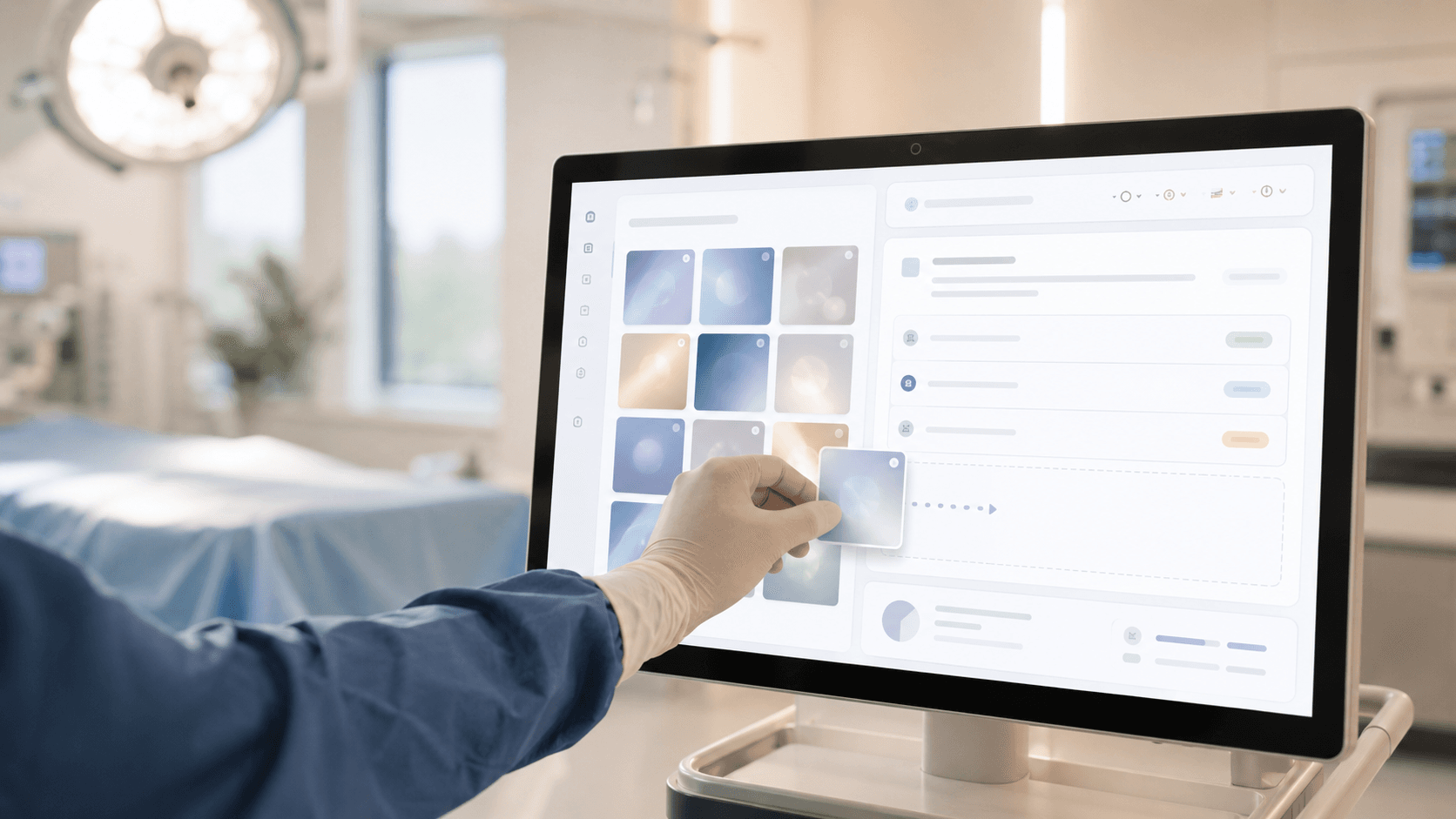
Image Selection Built In
Images captured during the procedure are available right inside the report builder, so the doctor can drop the relevant ones straight into the GP letter alongside the findings.
Report Ready at Recovery
As soon as the doctor finishes working through the procedure, the full report covering diagnosis, findings, and images is ready to print. Patients can leave with their procedure report in hand.
Who Benefits
Built for your team.
What to Expect
What to expect from ScribeWiz.
Built From the Procedure, Not After It
Most documentation tools start once the procedure is over. ScribeWiz builds the report as the doctor works through the procedure, so there's no separate dictation or typing step afterward.
Specialty-Specific Branching Logic
ScribeWiz only ever shows the gastroenterologist what is relevant. A gastroscopy never surfaces colonoscopy-only findings, and vice versa, keeping every report fast to complete and clinically precise.
ICD Coding Without a Coder
Statutory health-department reporting requires ICD codes for every diagnosis and finding. ScribeWiz attaches the correct code the moment the doctor selects the finding, removing a step hospitals would otherwise do by hand.
One Report, Every Format the Doctor Wants
Some doctors want a one-paragraph summary, others want a detailed multi-section letter. ScribeWiz is configured per doctor, so every gastroenterologist gets their own voice without compromise.
Connected to the Whole Procedure Record
Images captured during the procedure, the patient's theatre check-in details, and the final report all live in the same connected record, with no separate systems to reconcile.
Ready to see ScribeWiz in action?
Talk to our team about your practice's specific needs where we'll walk you through everything.